

FAMILIAL UNBALANCED REARRANGEMENTS
OF CHROMOSOME 5 DUE TO A MATERNAL
BALANCED TRANSLOCATION 5;9
Sukarova-Angelovska E, Kocova M*
*Corresponding Author: Professor Dr. Mirjana Kocova, Pediatric Clinic, Medical Faculty, Vodnjanska 17, 1000 Skopje, Republic of Macedonia; Tel: +389-111-713; Fax: 389-129-027; E-mail: ozonunit@unet.com.mk
page: 73
|
|
DISCUSSION
Reciprocal translocations of autosomal chromosomes are relatively common in the general population, usually without phenotypic expression in the carrier. They are usually detected after an unbalanced segregation in a carriers offspring occurs, or if one or both breakpoints of the translocation involve active genes.
There are many reports on the structural rearrangements of chromosome 5. The breakpoint of the short arm of chromosome 5 can be variable, extending from p13 to p15. The possible reason for the breakage of this part of chromosome 5 is a large number of repetitive elements in this region [6].
Efforts to make a genotype-phenotype map of this region have been made in order to elucidate the smallest region that is responsible for mental retardation and dysmorphic features [4,7,8]. Criteria for classification of eight types of CdCS have been suggested by some authors, depending on the breakpoints and the length of the deleted region [9].
Although the deletion of 5p is a common finding in cases with CdCS, the percentage of translocation (both de novo or familial) is not negligible (8-15%). Familial translocation occurs in 3% of all cases with CdCS. Many chromosomes are reported to be involved in a translocation together with chromosome 5. Case reports with translocations involving chromosomes 3q, 4p, 4q, 6q, 7p, 8p, 9p, 9q, 11q, 12q, 14q, 15q, 18p, 18q, and 22q have been published [10-30]. Chromosomes 10, 13, and 21, however, are the most frequently involved [3,31-37].
To the best of our knowledge, there is only one case, described by Monteleone et al. [19], with rearrangements between chromosomes 5 and 9, as in our family. In the literature concerning monosomies/trisomies 5p, significant excess of monosomic cases can be found, in comparison with trisomic cases. This is in concordance with the epistatic hypothesis for partial trisomies of chromosomes of group B. According to this hypothesis, trisomic fetuses derived from unbalanced familial translocations rarely survive the full gestational period, and are lost during the first few months of pregnancy [38].
Our case belongs to a very rare group with cases of both partial trisomy and partial monosomy 5p in the same family. Appearance of an unbalanced complement in an offspring of a balanced carrier is, according to some authors, a risk as high as 20% [39]. Sometimes, as in the above described family, this risk is even higher. The reported family had only two phenotypically normal children, but both were carriers of the translocation. Thus, a balanced translocation in the mother presented a very high risk for unbalanced offspring in this family. Such unbalanced translocations probably also occurred in the three deceased children, which will raise the risk in this family to 71% (5/7). The other two girls carry balanced translocations inherited from the mother, which further increases the risk for the next generations. There was no possibility of performing larger investigation of the karyotype in the mothers family, so the question as to whether her translocation was de novo or inherited remains unclear.
An additional question regarding the mother's balanced translocation 5;9 and thyroid cancer can be raised. Thus far, there is no data that breakpoints involved in the balanced translocation in this patient (5p14 and 9p24) could be associated with some of the cases with thyroid carcinogenesis. However, it remains to be elucidated in the future.
Due to the high risk to the offspring in families with translocations involving chromosome 5, genetic counseling is warranted. Parents should be informed about the possibilities of prenatal diagnosis, as well as other possibilities of conception that will decrease the risk.

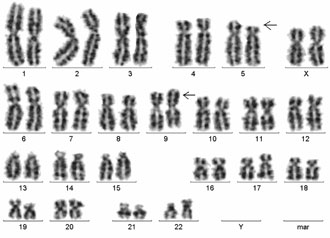

Figure 3. Partial karyotypes of A) the proband: del 5p; B) balanced translocation 5;9 in the mother and two healthy daughters; C) partial karyotype of the sister with trisomy 5p.
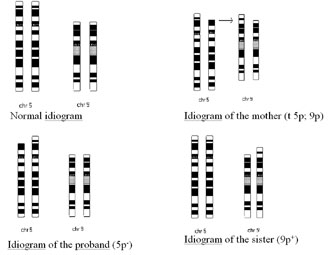
Figure 4. Idiogram of the karyotype in individuals of the family.
|
|
|
|

 |
Number 27
VOL. 27 (2), 2024 |
Number 27
VOL. 27 (1), 2024 |
Number 26
Number 26 VOL. 26(2), 2023 All in one |
Number 26
VOL. 26(2), 2023 |
Number 26
VOL. 26, 2023 Supplement |
Number 26
VOL. 26(1), 2023 |
Number 25
VOL. 25(2), 2022 |
Number 25
VOL. 25 (1), 2022 |
Number 24
VOL. 24(2), 2021 |
Number 24
VOL. 24(1), 2021 |
Number 23
VOL. 23(2), 2020 |
Number 22
VOL. 22(2), 2019 |
Number 22
VOL. 22(1), 2019 |
Number 22
VOL. 22, 2019 Supplement |
Number 21
VOL. 21(2), 2018 |
Number 21
VOL. 21 (1), 2018 |
Number 21
VOL. 21, 2018 Supplement |
Number 20
VOL. 20 (2), 2017 |
Number 20
VOL. 20 (1), 2017 |
Number 19
VOL. 19 (2), 2016 |
Number 19
VOL. 19 (1), 2016 |
Number 18
VOL. 18 (2), 2015 |
Number 18
VOL. 18 (1), 2015 |
Number 17
VOL. 17 (2), 2014 |
Number 17
VOL. 17 (1), 2014 |
Number 16
VOL. 16 (2), 2013 |
Number 16
VOL. 16 (1), 2013 |
Number 15
VOL. 15 (2), 2012 |
Number 15
VOL. 15, 2012 Supplement |
Number 15
Vol. 15 (1), 2012 |
Number 14
14 - Vol. 14 (2), 2011 |
Number 14
The 9th Balkan Congress of Medical Genetics |
Number 14
14 - Vol. 14 (1), 2011 |
Number 13
Vol. 13 (2), 2010 |
Number 13
Vol.13 (1), 2010 |
Number 12
Vol.12 (2), 2009 |
Number 12
Vol.12 (1), 2009 |
Number 11
Vol.11 (2),2008 |
Number 11
Vol.11 (1),2008 |
Number 10
Vol.10 (2), 2007 |
Number 10
10 (1),2007 |
Number 9
1&2, 2006 |
Number 9
3&4, 2006 |
Number 8
1&2, 2005 |
Number 8
3&4, 2004 |
Number 7
1&2, 2004 |
Number 6
3&4, 2003 |
Number 6
1&2, 2003 |
Number 5
3&4, 2002 |
Number 5
1&2, 2002 |
Number 4
Vol.3 (4), 2000 |
Number 4
Vol.2 (4), 1999 |
Number 4
Vol.1 (4), 1998 |
Number 4
3&4, 2001 |
Number 4
1&2, 2001 |
Number 3
Vol.3 (3), 2000 |
Number 3
Vol.2 (3), 1999 |
Number 3
Vol.1 (3), 1998 |
Number 2
Vol.3(2), 2000 |
Number 2
Vol.1 (2), 1998 |
Number 2
Vol.2 (2), 1999 |
Number 1
Vol.3 (1), 2000 |
Number 1
Vol.2 (1), 1999 |
Number 1
Vol.1 (1), 1998 |
|
|