

MICROSATELLITE INSTABILITY OF
COLORECTAL CANCERS IN PATIENTS
FROM THE REPUBLIC OF MACEDONIA
Stefanovska A-M1,*, Jasar D2,*, Zografski G2, Josifovski T3,
Panovski M3, Efremov GD1, Dimovski AJ1
*Corresponding Author: Dr. Aleksandar J. Dimovski, Macedonian Academy of Sciences and Arts, Research Center for Genetic Engineering and Biotechnology, Aven Krste Misirkov 2, POB 428, 1000 Skopje, Republic of Macedonia; Tel: +3892-120253; Fax: +3892-115434; E-mail: aleks@manu.edu.mk
page: 11
|
|
DISCUSSION
In this paper we describe the analysis of the MSI status in a cohort of colorectal cancer patients from Macedonia. The study was conducted with two different methods, nonradioactive PCR-PAGE and fluorescent multiplex PCR/capillary electrophoresis assay. Similar results were obtained with both methods, making the fluorescent multiplex PCR the method of choice for a routine MSI analysis due to its simplicity, speed and lesser manipulation requirements. From the five microsatellite markers used in this study, the BAT26 exhibited 100% sensitivity and 100% specificity in the detection of MSI-H phenotype in tumors. The sensitivity and specificity for D17S250, D18S61, D18S58 and DCC markers were 81.8 and 100%, 72.7 and 98.9%, 63.6 and 98.9%, and 45.5 and 98.9%, respectively. These data support the suggestion of Yamamoto et al. [20] that BAT26 can be used as a single marker for the detection of MSI status in colorectal tumors.
The frequency of MSI in our group of patients was 10.3% which is within the reported range in several extensive studies [11,21]. None of the tumors with the MSI-H phenotype had nodal involvement, and 10/11 of these were right sided (caecum, colon ascendens and transversum). These tumors were also associated with lower Dukes stage at diagnosis and primarily mucinous histotype. These data are in agreement with the general opinion about the histopathological characteristics and MSI status of colorectal tumors [21]. However, MSI status was not associated with age in our group of patients, contrary to several studies published recently [13,21]. Bearing in mind that HNPCC is generally associated with a younger age at diagnosis, in comparison with cases with the sporadic form of the disease, one of the possible explanations of this discrepancy is that there is a lower frequency of HNPCC carriers in our group of patients. Since this was a retrospective study, we did not have sufficient information on the family history of each patient, or enough material to conduct mutational analyses of MMR genes to clarify this issue. A prospective study is underway which should resolve this question in the near future.
Instability at only one locus was detected in three patients. In a recent study it was concluded that this type of instability can be detected in most, if not all, colorectal carcinomas, if a sufficient number of markers is used [17]. Other authors have presented evidence that the MSH6 gene inactivation is associated with MSI-L phenotype [22]. Since no detailed family history and no material for MSH6 gene analysis was available, it is difficult to discriminate between these two possibilities, and this issue will also be addressed in the ongoing prospective study.
Fig. 1. Detection of MSI phenotype at three loci by PCR-PAGE (left) and fluorescent PCR/capillary electrophoresis (right).
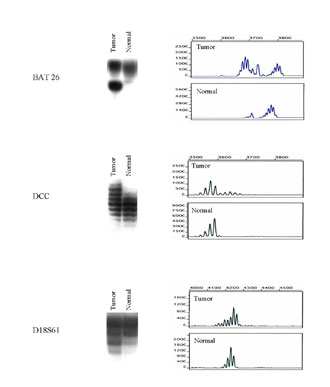
Table 1. MSI status for each of the seven markers in the 14 MSI positive tumors
030-02_1a.jpg)
Table 2. The frequency of MSI at the seven markers in MSI-H and MSI-L tumors
030-02_a.jpg)
Table 3. Association of MSI status and some clinical and histopathological features in 107 patients with colorectal cancer
030-02_3a.jpg)
|
|
|
|

 |
Number 27
VOL. 27 (2), 2024 |
Number 27
VOL. 27 (1), 2024 |
Number 26
Number 26 VOL. 26(2), 2023 All in one |
Number 26
VOL. 26(2), 2023 |
Number 26
VOL. 26, 2023 Supplement |
Number 26
VOL. 26(1), 2023 |
Number 25
VOL. 25(2), 2022 |
Number 25
VOL. 25 (1), 2022 |
Number 24
VOL. 24(2), 2021 |
Number 24
VOL. 24(1), 2021 |
Number 23
VOL. 23(2), 2020 |
Number 22
VOL. 22(2), 2019 |
Number 22
VOL. 22(1), 2019 |
Number 22
VOL. 22, 2019 Supplement |
Number 21
VOL. 21(2), 2018 |
Number 21
VOL. 21 (1), 2018 |
Number 21
VOL. 21, 2018 Supplement |
Number 20
VOL. 20 (2), 2017 |
Number 20
VOL. 20 (1), 2017 |
Number 19
VOL. 19 (2), 2016 |
Number 19
VOL. 19 (1), 2016 |
Number 18
VOL. 18 (2), 2015 |
Number 18
VOL. 18 (1), 2015 |
Number 17
VOL. 17 (2), 2014 |
Number 17
VOL. 17 (1), 2014 |
Number 16
VOL. 16 (2), 2013 |
Number 16
VOL. 16 (1), 2013 |
Number 15
VOL. 15 (2), 2012 |
Number 15
VOL. 15, 2012 Supplement |
Number 15
Vol. 15 (1), 2012 |
Number 14
14 - Vol. 14 (2), 2011 |
Number 14
The 9th Balkan Congress of Medical Genetics |
Number 14
14 - Vol. 14 (1), 2011 |
Number 13
Vol. 13 (2), 2010 |
Number 13
Vol.13 (1), 2010 |
Number 12
Vol.12 (2), 2009 |
Number 12
Vol.12 (1), 2009 |
Number 11
Vol.11 (2),2008 |
Number 11
Vol.11 (1),2008 |
Number 10
Vol.10 (2), 2007 |
Number 10
10 (1),2007 |
Number 9
1&2, 2006 |
Number 9
3&4, 2006 |
Number 8
1&2, 2005 |
Number 8
3&4, 2004 |
Number 7
1&2, 2004 |
Number 6
3&4, 2003 |
Number 6
1&2, 2003 |
Number 5
3&4, 2002 |
Number 5
1&2, 2002 |
Number 4
Vol.3 (4), 2000 |
Number 4
Vol.2 (4), 1999 |
Number 4
Vol.1 (4), 1998 |
Number 4
3&4, 2001 |
Number 4
1&2, 2001 |
Number 3
Vol.3 (3), 2000 |
Number 3
Vol.2 (3), 1999 |
Number 3
Vol.1 (3), 1998 |
Number 2
Vol.3(2), 2000 |
Number 2
Vol.1 (2), 1998 |
Number 2
Vol.2 (2), 1999 |
Number 1
Vol.3 (1), 2000 |
Number 1
Vol.2 (1), 1999 |
Number 1
Vol.1 (1), 1998 |
|
|